Dynamic Stability of Children Gait
Dan B. Marghitu and Eleonor D. Stoenescu
Department of Mechanical
Engineering, Auburn University, AL 36849, USA
Abstract. In this study we used the techniques of
nonlinear dynamics to analyze the stability of normal and pathological gait in
children. We based the analysis on the assumption that a human at steady state
locomotion can be represented as a nonlinear periodic system. Kinematic data
for the lower limb joints were used to construct phase plane portraits for the
hip, the knee and the ankle joints. Anomalies in the joint rotations of
pathological individuals were graphically depicted, by comparing the phase
plane portraits. Using the Floquet theory, an index of dynamic stability was
used to compare normal and pathological gait.
1 Introduction
The study of human
gait has been the culmination of numerous efforts in understanding the basic
principles underlying this phenomenon. These studies have a direct application
in the diagnosis of gait abnormalities and in their effective treatment. The
methodologies adopted for carrying out these studies have diverse origins and
have consistently evolved with developments in technology.
The first return map was used along with the phase plane portraits to
distinguish gait abnormalities in humans [1]. Along with these techniques, a
scalar measure that allowed for a comparison between the dynamic stability of
normal and post-polio gait was proposed [2]. In this study we base our analysis
on phase plane portraits, Poincaré maps and the Floquet multipliers [3]. We
analyze the stability of walking in children both normal and with pathological
disorders of the knee and ankle.
2 Human subjects and data collection
The study was carried
out over a subject population of six children belonging to the age group of 7-9
years. One of the subjects was classified as being perfectly normal with no
indications of any pathologic disorders. The remaining five subjects had
pathologic rotational disorders of the knee or ankle joints to a varying degree.
3 Mathematical background
The walking human
being can be then represented as a nonautonomous, periodically forced nonlinear
dynamical system, by a set of n first
order ordinary differential equations:
![]() (1)
(1)
where x is
a vector in the phase space <n. The vector
field F(.,t) = F(.,t+T) is periodic in time with a
period T. A set of solutions representing the walking patterns of the human
would then be given by
x(t)
= x(t + T) (2)
For the mathematical analysis of any such system, it
is required to identify a set of variables that describe the dynamics of the
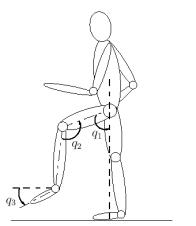
system. For this purpose we consider the simplified planar model shown in
Figure 1. For simplifying the analysis the joints are assumed to be purely
rotational with non-deformable members. Rotations of the hip joint (q1), the knee joint (q2), the ankle
joint (q3) and their corresponding angular velocities ![]() are selected as the
variables of state. The vector x can then be represented as
are selected as the
variables of state. The vector x can then be represented as
![]() (3)
(3)
|
|
The motion of this system would then evolve in
6-dimensional state space and the solutions can be studied by considering their
trajectories in the ![]() projections of this space. This task is
complicated by the fact that time appears as an additional coordinate, since
the system is nonautonomous. A simple way to overcome this difficulty is by
using the method of the Poincaré sections.
The technique involves placing fictitious planes transverse to the trajectories
in phase space at regular intervals and observing the points of intersection.
For further illustration, let us represent the trajectories of the system given
by Eq. (1) as G. We define a hyperplane S such that a) it is
always transverse to G and b) the trajectories always cross it in the same
direction. Also let the points of intersection of G with
S be represented by x0, x1, . . . , xk, . . .. The
Poincaré map would then be a continuous mapping M of S
into itself, such that
projections of this space. This task is
complicated by the fact that time appears as an additional coordinate, since
the system is nonautonomous. A simple way to overcome this difficulty is by
using the method of the Poincaré sections.
The technique involves placing fictitious planes transverse to the trajectories
in phase space at regular intervals and observing the points of intersection.
For further illustration, let us represent the trajectories of the system given
by Eq. (1) as G. We define a hyperplane S such that a) it is
always transverse to G and b) the trajectories always cross it in the same
direction. Also let the points of intersection of G with
S be represented by x0, x1, . . . , xk, . . .. The
Poincaré map would then be a continuous mapping M of S
into itself, such that
![]() (4)
(4)
As Eq. (1) has a unique solution, each intersecting point of G and S can be determined from the previous one. This would imply that a continuous-time evolution of Eq. (1) will be replaced with a discrete-time mapping, by the Poincaré section. To analyze the stability of these trajectories we insert the Poincaré sections at well defined instances of the gait cycle. For a human being in locomotion, each cycle would be defined as the motion achieved in between successive foot contact events of the same limb. A choice of events could be the heel strike, heel off, toe on and toe off or even the instant of maximum flexion of the knee joint. Choosing the instant of maximum flexion of knee joint for inserting the Poincaré map Eq. (1) can be represented by
![]() (5)
(5)
where, the subscript kf denotes maximum knee
flexion, xk and xk+1 represent
the vector sampled at the instant of maximum knee flexion during the kth and k + 1th cycles
respectively. The stability of the closed orbit can then be determined with
respect to infinitesimal perturbations d. The Poincaré map Mkf is then
linearized in the neighborhood of xe and is described by
 (6)
(6)
where the J is known as the Jacobian or the
Floquet matrix. The stability of the above system can be studied by observing
the eigenvalues of the Floquet matrix (represented by lj, j
= 1, 6). To visualize this idea in a better manner let us rewrite the above
equation in a different form. The linearized system after one period can be
represented as
![]() (7)
(7)
where the image of a point xe + d
which initially was in the neighborhood of xe is now at a distance. After m periods the
system is represented by the expression
![]() (8)
(8)
where the initial displacement d is
multiplied by Jm . If the
eigenvalues of J (also known as the Characteristic multipliers) are less
than one in magnitude, then any displacement from the fixed point xe decreases
exponentially and the periodic trajectory is asymptotically stable. On the
other hand if the magnitude of any of the eigenvalues is larger than one, the
displacement would grow exponentially and the trajectory would be unstable. If
we compare the gait of two subjects who have all their multipliers within the
unit circle, the gait of the subject with the larger multiplier will be less
stable than that of the other. Utilizing this property, we define a scalar
measure of gait stability as,
![]() (9)
(9)
The system under consideration is a human being system
and the analytical representations of the function Mkf and the matrix J are extremely difficult to
obtain. However, we can estimate J from experimentally acquired
kinematic data [1, 2] using curve fitting techniques. This estimation of J
is then used to compute the g-measures.
4 Results
|
Fig. 2 Phase plane portraits for the
subject with normal gait and the portraits for three of the subjects with
pathological gait |

Kinematic data of the hip joint (q1), the knee joint (q2) and the
ankle joint (q3) were
defined in the saggital plane and collected using a video based motion analysis
system for a minimum of 5 gait cycles. Each gait cycle was defined as the
motion achieved between consecutive heel strike events of the same foot. The
joint rotation data for all three joints were numerically differentiated to
obtain the corresponding velocities and both quantities were averaged over the
five cycles. Phase plane portraits for each joint were obtained by plotting
these averaged joint rotations against their respective velocities. The instant
of heel strike was also averaged and plotted on the phase plane portraits.
Figure 2 depicts phase plane
portraits for the subject with normal gait along with the portraits for three
of the subjects with pathological gait. The fact that all the phase
trajectories on the portraits are closed loops indicates that the joint
movements are periodic. The Floquet multipliers for the normal and pathological
subjects were computed from the Jacobian matrix and depicted on the complex
plane.
|
Fig. 3 Floquet multipliers on the complex plane |
The multipliers for all subjects
were less than one in magnitude. Relative stability of gait for all subjects
was quantified by comparing the magnitudes of their largest multipliers, which
was defined as the g measure. The g measure for the subject with normal
gait had a value of 0.47. The measures for all the pathological subjects were
compared with that of the normal and were found to vary from 0.55 to 0.78,
Figure 3.
This would imply
that the gait of all five pathological subjects is more unstable than the gait
of the normal subject. Also the subject with a g
measure of 0.78 has the most unstable gait as compared to all the other
subjects.
References
[1]
Y. Hurmuzlu
et al., “Presenting joint kinematics of human locomotion using phase plane
portraits and the Poincaré maps”, J.
Biomech. 27 (12), pp. 1495, 1994.
[2]
Y. Hurmuzlu
and C. Basdogan, “On the measurement of stability in human locomotion”, J.
Biomech. 116, 30 1994.
[3] A. H. Nayfeh and B. Balachandran, Applied Nonlinear Dynamics, John Wiley & Sons, Inc., New York, 1995.
![]()